



Decisions Ahead: The State of Academic Medicine
Even before the NIH IDC rate drop was announced on Friday, many academic medical centers were already struggling. So what now?


This weekend, I fully intended to focus this post on medical innovations, which is the reason I started this Substack in the first place. And it will. Just not today. Or perhaps not in the way I had initially intended it. Suppose we define innovation as introducing new ideas or methods. In that case, then today I am compelled to discuss the challenges that Academic Medical Centers (AMCs) face and the innovations we will need to save them.
So, where does this story begin? On Friday, the NIH announced a drop in their indirect cost rate (IDC) to a flat 15%. By Friday evening, my phone was blowing up with text messages. The newswires finally picked up the story. But talking to the average citizen, the implications aren’t obvious. On Saturday, I tried to explain the situation to a friend. After 15 minutes, I think she got it… maybe. So, I want to explain what IDCs are, but we need to discuss something even more critical. AMCs were already in trouble even before this announcement.
The Boring but Important Part: What Are IDCs?
So, let’s start with the bomb that got dropped on Friday. Indirect costs (IDCs), also referred to as "Facilities and Administrative" (F&A) costs, are essential components of research funding. These costs support the infrastructure that makes research possible: buildings and facilities (labs and offices), utilities and IT infrastructure (keeping the lights on and the internet working), and administrative services that process grant awards and ensure compliance with complex regulations. An infographic from the Association of American Medical Colleges that helps to explain this is available here and shown below.
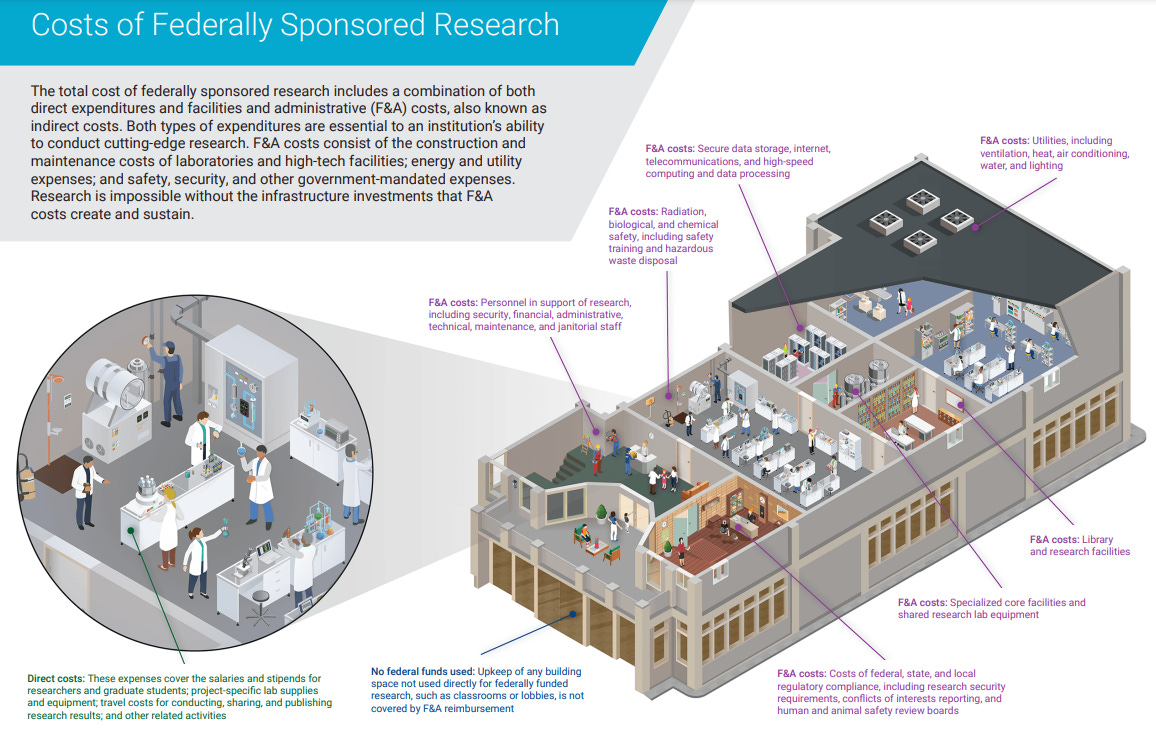
The application and submission processes for NIH grants are incredibly complex, as are the regulations accompanying them. Significant human infrastructure is required to support these processes. Many items necessary for research—such as lab space, equipment, and safety oversight—aren’t even allowed as part of the “direct costs” portion of the budget, which typically only covers salaries and supplies specific to the proposal. The federal government has long recognized that IDCs help defray these additional expenses.
IDC rates are set on an institution-by-institution basis through a detailed proposal outlining the actual indirect costs incurred. This negotiation typically occurs every three to five years to set an institution’s IDC rate. When a scientist submits a budget to the NIH, IDCs are added on top of the direct costs. I get it; when anyone outside the field hears that IDCs are often between 50-70%, it sounds exorbitant. But it's partly because of the many things required to do the research that aren’t allowable in the direct cost budgets.
And here is perhaps the most shocking fact of all. If we add the direct and indirect costs, we still don’t come close to fully covering the actual research costs. I’ve discussed this with experts from various institutions who have told me that for every federal research dollar received, it costs the institution another 50-60 cents to do the work. According to the AAMC website, colleges and universities paid $27.7 billion of their own funds toward academic R&D in FY23, including $6.8 billion in unreimbursed F&A costs. The bottom line is that even with the IDCs, conducting NIH-funded research in the U.S. was already a money-losing business.
Wait, what?
You might be asking yourself, how is this even sustainable? It’s not. The only way this has been possible is through a complicated “funds flow” model where AMCs use clinical revenue and other sources, like donations, to subsidize research and teaching. Physicians and staff at AMCs believe in their mission: discovering cures, educating the next generation of physicians, and caring for patients. However, AMCs were already under significant financial strain even before this IDC announcement. Between 2008 and 2020, AMCs experienced a 123% increase in operating expenses while revenue grew by only 110%. Since the pandemic, inflation has exacerbated these pressures, with rising medical supplies and wage costs. At the same time, third-party payers continue to push to reduce reimbursements for clinical services. Clinical margins are tighter than ever, making it increasingly challenging to subsidize research expenses. Adding a flat 15% IDC rate to the mix renders the situation untenable.
Why It Matters
For “fun,” a colleague of mine asked chatGPT what the natural consequences of this decision would be. “A 15% flat IDC rate would be devastating to US biomedical research. It would force institutions to cut research support, push financial burdens onto physicians, drive scientists out of academia, and shift US research leadership toward industry and foreign competitors. After four years, the consequences would be severe but survivable. After that, the consequences would be devastating and permanent.” You get the picture.
There’s a lot on the line. AMCs serve critical roles in our health system: providing patients access to clinical trials, driving cutting-edge basic science, creating the next generation of doctors, and fostering environments where experts can innovate. If you’ve ever known someone with a severe or rare disease, AMCs are the first place to go for help. Without them, such patients would have nowhere to turn.
We also must not forget that academic medical centers directly employ roughly 2.7 million people. However, only a tiny fraction of those people are MDs or PhDs. The majority are administrative, clinical, research, and maintenance staff who would lose their jobs if the system implodes, not to mention the patients who would lose access to healthcare and the students who would not be trained to be our healthcare professionals of the future.
What’s the Solution?
Well, I can tell you that the proposed 15% IDC flat rate isn’t it. Policymakers need to confront the actual costs of research. Essential infrastructure, like institutional review boards that review clinical trials for safety and ethics, secure data storage, and advanced facilities, do not come cheap. If IDCs are not to cover these costs, they will need to go into the direct expenses, and budgets will have to accommodate to allow for them. The size of a standard R01 application ($500K in annual direct costs) hasn’t changed since October of 2001. Yet, salaries and supply costs have all risen significantly since then, as have the complexities of the grant application processes.
So what could bring costs down? Could AMCs run leaner? Of course, they could. However, to bring IDCs down and make AMCs more financially viable, meaningful innovations are needed from both the NIH and AMCs. Grant applications are a notorious source of administrative burden. Many run hundreds or even thousands of pages and take months to complete. Simplifying these processes would reduce costs and free up researchers to focus more on their science rather than paperwork. While regulatory oversight is critical for ensuring safety and ethical standards, there is significant redundancy in the current system. The grant application, management, and compliance tracking systems could be significantly simplified, reducing costs for the NIH and the institutions that partner with them.
But AMCs will also need to adapt. The good news is that AMCs aren’t just sitting around waiting for a miracle. Many are already rolling up their sleeves. Expanding research portfolios to include greater collaboration with industry is a place where many have already started. Operational efficiency is also a no-brainer. Many AMCs have focused on expanding their regional networks and buying up other hospitals. This allows greater leverage with insurers and suppliers while providing economies of scale for administrative systems.
Telemedicine is another example. As long as CMS funds it, virtual healthcare helps AMCs reach patients in underserved areas while generating funds. But this concept can extend way beyond “virtual visits.” Mayo Clinic has perhaps been one of the most successful at doing this. They generate revenue by charging membership fees to over 40 aligned practices for access to its tools and expertise, such as eConsults and digital platforms. Mayo also offers consulting packages for hospitals that are building "hospital at home" programs. They also developed a global reference laboratory that performs 25 million tests annually, serving 4.5 million patients worldwide.
Michigan Medicine recently expanded specialty pharmacy services, focusing on higher-cost biologic therapies that are more complicated to get approved and administer. By moving this program “in-house” for most Michigan Medicine patients, everybody gets better service, and everybody wins.
While a much more controversial option, some health systems are increasingly collaborating with AI companies, sharing patient data to advance the development of AI-driven health tools. Ethical issues abound, but STAT has a good recent article here if you’d like to read more. Due to the financial realities, more health systems will likely be willing to consider this option as an additional revenue stream.
The Bigger Picture
The NIH’s proposed 15% IDC rate is a gamble with the future of American health research, care, and education. AMCs are more than just research hubs; they are vital to the nation’s health, economy, and global leadership in science. These institutions are one of America’s greatest treasures. AMCs provide patients access to cutting-edge clinical trials and groundbreaking treatments, train the next generation of physicians, and anchor the research efforts that fuel medical breakthroughs and economic growth.
But, yes, the long-term survival of AMCs will require transformation—one defined by strategic adaptation and reinvention. AMCs will need to become leaner and more efficient; they will need to explore and expand revenue streams and, frankly, consider creating more powerful healthcare networks by partnering with each other. Most importantly, they will need time to get there, and NIH funding must continue to account for the actual cost of research. The path forward will not be easy, but the stakes are too high to risk undermining these vital institutions. The future of American health hangs in the balance.
The path forward is better selection of impactful grants, better selection of PIs with integrity and competence, and the dismantling of the cabal of peer review funding!!
Cutting “administrative” Indirects is a direct hit on dismantling that bureaucracy.
Letting PIs take over the spending of indirects is most likely to be effective in propelling impactful research forward, AND for researchers to have a greater say in the direction of research institutes.